
Author: Dr. Xiao Chi (Tony) Zhang, Alpert Medical School of Brown University, Residency in Emergency Medicine, on behalf of the CORD Student Advising Task Force.
This is the second post in a series on Special Advising Circumstances, following the previous post on the Military Match in Emergency Medicine. The purpose of this series is to disseminate the collective wisdom of EM clerkship and program directors on how to navigate advising students at greater risk to not match in EM. The author would like to thank Dr. Hillman, Dr. Kellogg, Dr. Kenney, and Dr. Edens for their contribution to this post.
General Overview of the IMG Application Process
International medical graduates (IMG) comprise physicians who have completed their training from a medical school outside from where they intend to practice. While IMG applicants can offer a wealth of cultural, academic, and medical knowledge diversity to a domestic residency program, many are facing increasing fundamental challenges during their application process. Historically, the number of available Emergency Medicine (EM) residency positions has exceeded the number of US senior applicants, allowing IMG’s, and other “non-traditional” applicants to fill in these gaps. However, recent data suggest that the number of IMG applications have tailed off in the last few years over a change in perceived competitiveness, despite the fairly stable rate of EM spots filled by US allopathic seniors. Furthermore, unlike U.S. graduate students, IMG’s must first complete the United States Medical Licensing Examination (USMLE) and then undergo a rigorous accreditation process by the Educational Commission for Foreign Medical Graduates (ECFMG) before they can apply for US residencies; only about half of the ECFMG applicants are certified.
The simple truth of the matter is that applying for EM Residency as an IMG is tough. The odds are stacked against them. Much of the standard application advice does not apply to their situation. In order to successfully match they need to know the rules of how the process works for IMG’s.
The primary goal of this post is to address the aforementioned hurdles for IMG applicants with both objective data from the National Residency Match Program (NRMP) and subjective recommendations, collected from EM program directors and clerkship directors on how to maximize your chances of successfully enrolling in an US EM Residency Program.
Before you choose EM
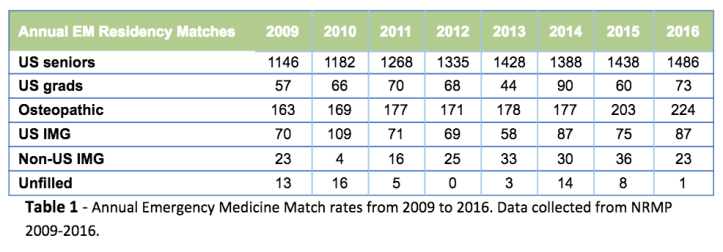
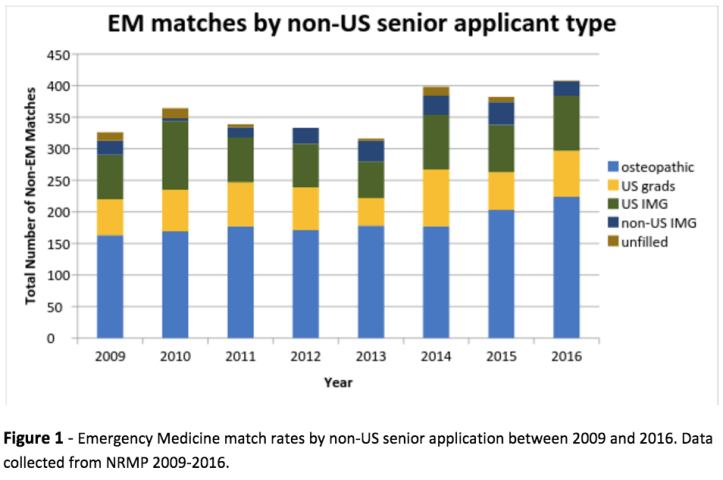
Prior to applying, it is important to set realistic expectations. Matching into EM is more difficult for International Medical Graduate (IMG) students than for United States (U.S.) students [see Table 1 and Figure 1]. According to the Results and Data from the 2016 Main Residency Match there were 1895 emergency medicine PGY-1 positions with 2476 total applicants. Of those, 783 were “independent applicants” (31.6%), which includes those who went to international medical schools. EM had a 99.99% fill rate with only 1 unfilled position. Approximately 78% of those spots were matched to US allopathic seniors and 12% were filled by osteopathic applicants. This adds up to some sobering news for the international applicant; only 5% of available EM positions were filled by US-IMG’s and 1% by non-US citizen IMG’s. This left 30% of independent applicants unmatched among those who listed EM as their only specialty.
Knowing the data is helpful, but to really know their chances as an applicant they need personalized advising. If their school does not have connections to advisors that are knowledgeable about the EM application process, the best option is to request an advising session with the program director or clerkship director at their first EM rotation. Most will be happy to meet and answer questions about the application process.
“Take-Away” Points from Away Rotations
One of the most important goals as an EM applicant is to secure a Standardized Letter of Evaluation (SLOE) during an away rotation in the emergency department. According to the 2016 NRMP Program Director Survey results, EM Program Directors ranked “Letters of Recommendation” as the #1 factor (97%) in their decision to offer an interview. And “Letters of Recommendation” was ranked as the #5 top citing factors (88%) with a Mean Importance Rating of 4.7 out of 5.0 for each factor when assembling their rank list.
Unfortunately for IMG applicants it can be difficult to secure the EM rotations that provide the kind of letters they need. Many programs reserve the coveted slots (July, August and September) for students from their affiliated medical school. Hospitals may also bar international rotators entirely, or only allow them from schools where they have a pre-existing relationship. To find viable rotation options the first step is to look at where students have rotated in the past. The second place to look is at the match list for foreign schools – see where IMG’s have matched and contact those departments about a rotation. The last, and unfortunately the most common way, is to call the departments where they are interested in rotating (and potentially applying to) to see if you can secure a rotation. This is time consuming and frustrating but may be necessary.
Rotations at non-academic emergency departments may be easier to obtain and they may be willing to write a letter of recommendation. However, these letters will not carry sufficient weight to get interviews. All applicants, not just IMG’s, need at least one (and preferably two) SLOEs from emergency departments with residency programs. The SLOE is far more useful to program directors than a regular LOR because it forces the writer to compare and contrast the applicant with their peers. Not having a SLOE will severely limit your chances as an applicant.
The Application
ERAS opens on September 6th, with programs able to view applications on September 15th – therefore the application needs to be complete as close to the 15th as possible. An IMG applicant will not receive interview offers until they have at least one SLOE uploaded. They should also take Step 2 early enough to have their scores back when applications go out. While US students may be able to delay Step 2 and still secure interviews, IMGs really need to have both Step 1 and Step 2 scores to maximize their chances of securing interviews. Choose to apply to programs that have matched IMG’s over the past few years (do this by looking at the match lists published by the schools and at the residencies websites). Applying to programs with no history of matching IMG’s is lower yield.
An IMG applicant should anticipate not having a large number of interview offers early in the applications season (late October/early November). It is okay to call program coordinators and to email program directors. They should be cautious not to cross the line from enthusiastic to overbearing or demanding. And they need to be prepared to do interviews later in the cycle (January) and to be ready to go on short notice. Though they are scheduled in a rush, these interviews carry just as much weight as any other.
The realistic IMG applicant will both apply broadly for emergency medicine but also apply for other specialties as well. They should not anticipate being able to scramble into EM. Vanishingly few (if any) international applicants (or anyone else for that matter) have matched via SOAP (Supplemental Offer and Acceptance Program) into EM.
The Interview
Obtaining an interview is a big step in the right direction. They still need to really shine in front of a program in order to match. If you have a unique background, use it to your advantage and highlight your qualities and experiences that make you ideal to train. Most importantly, be prepared to address your IMG status. Expect the question, “Why didn’t you go to medical school in the U.S.?” Have a good, honest answer.
The Rank List
IMG applicants with a longer contiguous rank list (the number of programs ranked in the first-choice specialty before a program in another specialty appears on the applicant rank order list) have a better chance of matching into EM residency than applicants with shorter contiguous rank lists. The more interviews they do (and the more programs they rank), the more likely they are to match.
Matched US-IMG and Non-US IMG applicants had a mean rank list of 6.2 and 4.1 respectively as opposed to the non-matched US-IMG and Non-US applicants had a mean rank list of 2.4 and 2.9 respectively. Although no number of interviews guaranteed a 100% match rate, the standard recommendation is to rank 12 programs (the matched US allopathic seniors had an average rank list consisting of 12.3 programs). In ordering programs on their list, it is important to not try to outsmart the algorithm: the match is applicant-weighted. IMG applicants should rank just like everyone else, based on where they want to go.
Final Thoughts and Frequently Asked Questions
Why are IMG applicants at a disadvantage?
- In general, U.S. graduate students who attend international medical schools are considered higher academic risks and held at a higher level of scrutiny since program directors have to determine why these students were not able to obtain a position in the United States. Any academic difficulty from a US graduate student at a foreign medical school is a major red flag and warrants a back-up plan.
- Non-US graduate students who were never US grads/citizens/students may be a different cohort, but it is challenging for US EM Program Directors to be familiar with the myriad of international medical schools. As a result, non-US IMG students need to demonstrate objective mastery of the medical arts via top grades, strong letters of recommendation (at least one SLOE), above average USMLE scores, and a robust CV.
- Due to these concerns many programs consider the presence of IMG residents to be a sign that a program is less competitive. This alone will prevent many programs from considering foreign trained applicants.
Are there financial implications to hiring an IMG resident?
- Unfortunately, yes. Some medical institutions only sponsor certain types of Visas, and for others, the Department has to pick up the tab. It is difficult for a PD justify spending money to match an IMG applicant when they can match an equally qualified US graduate for free.
What is one major pitfall for IMG applicants?
- Spelling and grammatical errors. Unfortunately, PD’s are bombarded with thousands of applications from highly qualifying applicants during the interview season. Any simple grammatical mistakes or typo on your documentation may reflect (possibly inaccurately) your level of English proficiencies and lead to rejection.
- Advice: have someone read your application, and then have someone read it again.
HIGH YIELD! What can IMG applicants do to tip the scale in their favor?
- Find a mentor and advisor to guide you through this challenging, but exciting process.
- Do some research first.
- Find out where your senior colleagues applied/rotated/matched and ask for their advice.
- Apply (although not exclusively) to programs that have a history of accepting IMG applicants.
- Rotate at an academic program and get an outstanding SLOE
- Speak/write proper English and make sure your ERAS application is flawless.
- Have an overall strong ERAS application:
- Appear special
- Include your unique services, leadership, and research.
- Don’t forget to mention your particular background. After all, you are going against major odds by applying to an EM residency program as an IMG, so demonstrate to the PDs that you are not afraid of a challenge.
- Make sure you have the right VISA for the institution that you are applying to.
- Have an advocate: financial, educational, or emotional (or all three).
What is our one big piece of advice to an IMG applicant?
- Before you apply to any EM programs, make sure you are the best possible candidate, having crossed all of your “t’s” and dotted your “i’s” before clicking the submit button.

Nice blog thanks for poosting
LikeLike